

 Registration successful
Registration successful Account activated – pending validation.
Account activated – pending validation. Your account has been activated successfully, but we still need to validate you as a healthcare professional. We’ll send you an email with the result of the validation process in the next [five] days.
Your account has been activated successfully, but we still need to validate you as a healthcare professional. We’ll send you an email with the result of the validation process in the next [five] days. In the meantime, you can enjoy access to all the latest news, events and resources on our website
In the meantime, you can enjoy access to all the latest news, events and resources on our websiteMESILICO suggests that Nucala offers potential for disease modification3
Influence of Nucala (mepolizumab) on Airway Remodeling in Severe Eosinophilic Asthma3
Type 2 inflammation is at the root of four underlying disease processes in severe asthma1-9, of which IL-5 is one of the central cytokines.10-17

Results of the MESILICO study
In addition to its marked clinical benefit, Nucala also results in a decrease in markers of airway remodeling, indicating a disease-modifying effect. 3

Histopathological findings
Average values from paired biopsies (n=34)
Improvement of bronchial epithelium integrity

Damaged/damaged epithelium,
p < 0.001

Airway smooth muscle area,%
p < 0.001
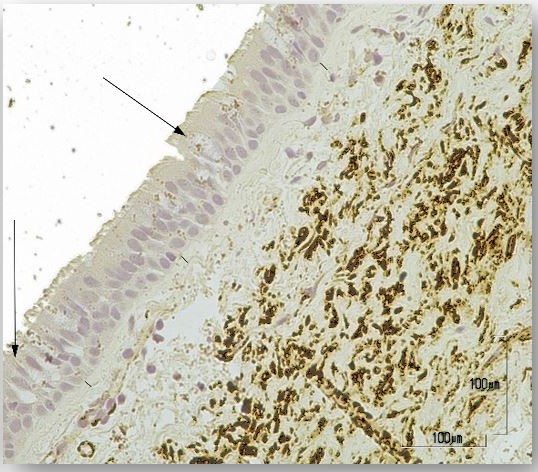
Representative endobronchial biopsy samples
Before mepolizumab
(initial situation)
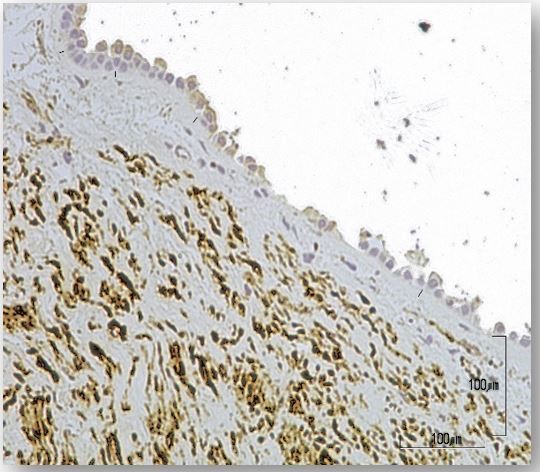
After mepolizumab
(12 months)
Domvri K, et al. J Allergy Clin Immunol. 0.017 2024, supplementary data 18
Respiratory tract, in mm. Before treatment with mepolizumab, a damaged respiratory epithelium is predominantly observed, peeling off.
After treatment with mepolizumab, a high percentage of intact and normal epithelium is observed. The surface of airway smooth muscle (in brown) has also decreased.
Reduction of the thickness of airway smooth muscle

Thickness of the layer of smooth muscle cells in the airways, in mm
p < 0.001
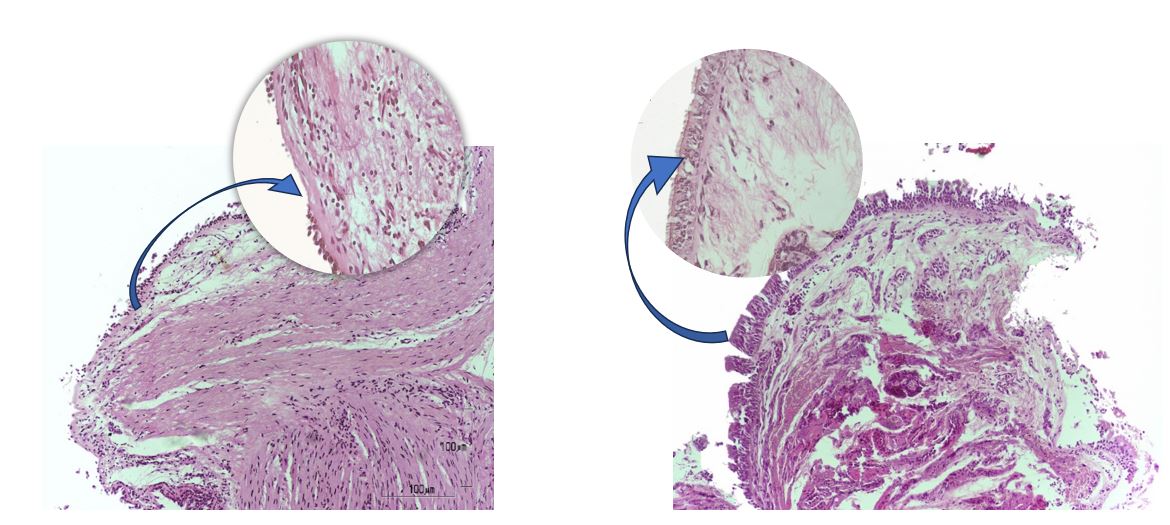
Before mepolizumab
(initial situation)
After mepolizumab
(12 months)
Domvri K, et al. J Allergy Clin Immunol. 0.017 2024, supplementary data 18
Damaged epithelium that detaches, along with a high percentage of areas showing smooth muscle hyperplasia.
After the administration of mepolizumab, a reduction in the thickness of the smooth muscles of the airways is observed, along with a significant proportion of intact epithelial, submucosal, and muscular tissues.
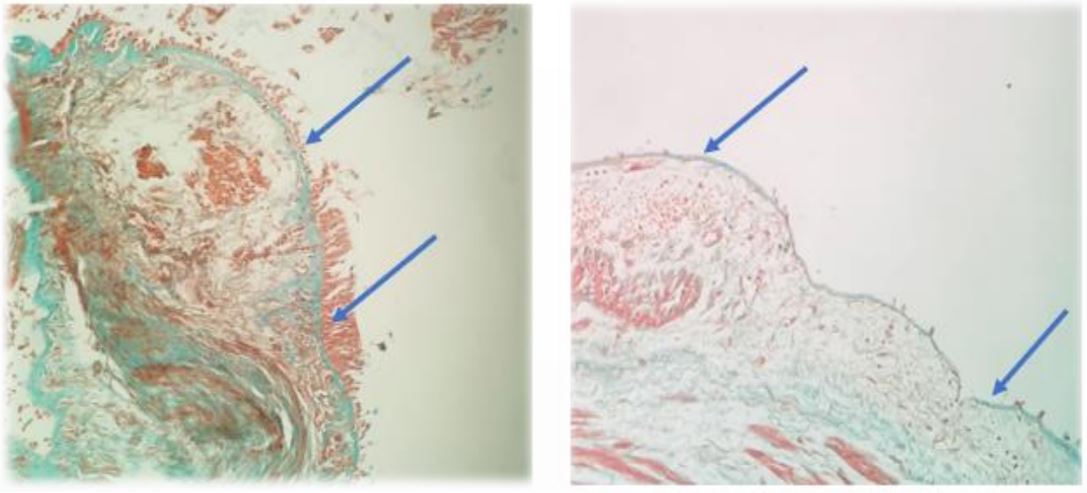
Reduction of the thickness of the sub-basement membrane

Thickness of the subbasal membrane, in μm
p < 0.001
Before mepolizumab
(initial situation)
After mepolizumab
(12 months)
Before mepolizumab
(initial situation)
After mepolizumab
(12 months)
Domvri K, et al. J Allergy Clin Immunol. 2024, supplementary data 18
Before treatment with mepolizumab, a thickened sub-basement membrane is observed.
After treatment with mepolizumab, the thickness of the airway basement membrane decreased.
* Values of p < 0.05 were considered statistically 24.4% significant. ** of the difference 26.0% matched mean.
Clinical Outcomes (N=39)
Clinically Significant Improvements: (p < 0.001)*
67 %
reduction
severe exacerbations – 2.1 to 0.7 per year
3.4 points
increase**
of the ACT score – from 18.4 to 21.8
10.5 %
upside**
FEV1 (% of initial value) – 69.5% to 80%
280 mL
upside**
FEV1 – 2.0 to 2.3 L

Summary
The MESILICO study suggests that Nucala presents, in addition to clinical improvements, 3 A potential for disease modification in severe eosinophilic asthma.
The MESILICO study examines patients with severe eosinophilic asthma in a clinically significant real-world population and provides insights into a possible central role of IL-5 in structural airway remodeling. 3
The results highlight the potential of biologics to positively influence disease progression in severe eosinophilic asthma. 3
Security Profile ‡
The safety profile of Nucala (mepolizumab) shows good tolerability and long-term safety. The results of a ten-year open-label extension study confirm this profile 19 and did not reveal any new security issues.
3 Criteria for inclusion in the study
Severe late-onset eosinophilic obstructive asthma
- Late onset occurs when the disease occurs after the age of 20.
- Obstructive character is defined by a post-bronchodilator FEV1/FVC ratio < 0.7.
- History: ≥ 1 exacerbation in the past year despite treatment with high-dose ICS/LABA or ISC/LABA/LLAMA
- Blood eosinophil (BEC) levels ≥ 150 cells/ μ L at screening or ≥ 300 cells/ μ L in the past 12 months
A full overview of the inclusion criteria on clinicaltrials.gov can be found under study number NCT04612556 (accessed 07/07/2025).

Participants were recruited from
8 Specialized
Asthma Centers
in Greece.
Footnotes
*Nucala is generally well tolerated. In clinical trials, Nucala had a similar incidence of adverse events vs. placebo with the exception of injection site reactions (8% vs. 3%), which occurred mainly within the first 3 injections.2
†The long-term safety and immunogenicity profile of Nucala was similar to that observed in placebo-controlled asthma trials.1
Real-world studies are designed to evaluate associations among variables and not to definitively establish causality. These limitations are important when interpreting results: lack of comparator arm, differences in patient populations and data collection vs. randomised controlled trials.8
The recommended dose of Nucala is 100 mg SC once every 4 weeks in adults and adolescents 12 years and older, available in a pre-filled pen, pre-filled syringe or lyophilised powder. The licensed dose of Nucala in children aged 6–11 years is 40 mg SC regardless of weight and available in lyophilised powder.2
AE, Adverse event; ATU, Temporary Authorization for Utilization; PT, preferred term; SAE, Serious adverse event; SC, subcutaneous; SOC, System Organ Class.
Abbreviations:
ACT – Asthma Control Test;
BEC – Blood Eosinophil Count; ICS – inhaled corticosteroids;
FVC – Forced Life Capacity;
LABA – Long-Acting Beta Agonists;
LAMA – Long-Acting Muscarinic Antagonists;
MESILICO – Efficacy of Mepolizumab in patients with latE-onset SevereeosInophiLic asthma and fIxed obstruCtiOn; s. c. – subcutaneous;
FEV1 – maximum expiratory volume in one second (forced capacity in one second).
‡ No safety data were collected in the MESILICO study3,18
Disclaimer:
The MESILICO study was conducted within the scope of Nucala's authorized indications. The available data do not indicate any additional benefit beyond the authorized indication.
References
- Raby KL, Michaeloudes C, Tonkin J, Chung KF, Bhavsar PK. Mechanisms of airway epithelial injury and abnormal repair in asthma and COPD. Front Immunol.
- Russell RJ, Boulet LP, Brightling CE, et al. The airway epithelium: an orchestrator of inflammation, a key structural barrier and a therapeutic target in severe asthma. Eur Respir J. 2024; 63(4):2301397.
- Domvri K, Tsiouprou I, Bakakos P, Steiropoulos P, Katsoulis K, Kostikas, K. Effect of mepolizumab in airway remodeling in patients with late-onset severe asthma with an eosinophilic phenotype. J Allergy Clin Immunol. 2025; 155(2):425- 435.
- Hewitt RJ, Lloyd, CM. Regulation of immune responses by the airway epithelial cell landscape. Nat Rev Immunol. 2021;21:347-362.
- Dunican EM, Watchorn DC, Fahy JV. Autopsy and imaging studies of mucus in asthma: lessons learned about disease mechanisms and the role of mucus in airflow obstruction. Ann Am Thorac Soc. 2018; 15(suppl 3):S184-S191. Benefits of Mepolizumab in Severe Asthma." CHEST Pulmonary 3.1 (2025): 100107.
- Dunican EM, Elicker BM, Gierada DS, et al. Mucus plugs in patients with asthma linked to eosinophilia and airflow obstruction. J Clin Invest. 2018; 128(3):997-1009.
- Chan R, Duraikannu C, Lipworth B. Clinical associations of mucus plugging in moderate to severe asthma. J Allergy Clin Immunol Pract. 2023; 11(1):195-199.e2.
- Siddiqui S, Bachert C, Bjermer L, et al. Eosinophils and tissue remodelling: relevance to airway disease. J Allergy Clin Immunol. 2023; 152(4):841-857.
- Varricchi G, Brightling CE, Grainge C, Lambrecht BN, Chanez P. Airway remodelling in asthma and the epithelium: on the edge of a new era. Eur Respir J. 2024; 63(4):2301619.
- Buchheit KM, Lewis E, Gakpo D, et al. Mepolizumab targets multiple immune cells in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. 2021; 148(2):574-584.
- Barretto KT, Brockman-Schneider RA, Kuipers I, et al. Human airway epithelial cells express a functional IL-5 receptor. Allergy. 2020; 75(8):2127-2130.
- Bergantini L, d’Alessandro M, Cameli P, et al. Regulatory T cell monitoring in severe eosinophilic asthma patients treated with mepolizumab. Scand J Immunol. 2021; 94(1):e13031.
- Maspero, Jorge et al. Type 2 inflammation in asthma and other airway diseases. ERJ open research vol. 8,3 00576-2021. 1 Aug. 2022.
- Howell I, Howell A, Pavord ID. Type 2 inflammation and biological therapies in asthma: targeted medicine taking flight. J Exp Med. 2023; 220(7):e20221212.
- Ueki S, Konno Y, Takeda M, et al. Eosinophil extracellular trap cell death–derived DNA traps: Their presence in secretions and functional attributes. J Allergy Clin Immunol. 2016; 137(1):258-267.
- Bajbouj K, AbuJabal R, Sahnoon L, Olivenstein R, Mahboub B, Hamid Q. IL-5 receptor expression in lung fi- broblasts: potential role in airway remodeling in asthma. Allergy. 2023; 78(3):882-885.
- Zhu Y, Bertics PJ. Chemoattractant-induced signaling via the Ras–ERK and PI3K–Akt networks, along with leukotriene C4 release, is dependent on the tyrosine kinase Lyn in IL-5– and IL-3–primed human blood eosin- ophils. J Immunol. 2011; 186(1):516-526.
- Domvri K, Tsiouprou I, Bakakos P, Steiropoulos P, Katsoulis K, Kostikas, K. Effect of mepolizumab in airway remod- eling in patients with late-onset severe asthma with an eosinophilic phenotype. J Allergy Clin Immunol. 2025; 155(2):425-435 (supplementary data).
- Pavord I et al. Long-term safety of mepolizumab for up to ~10 years in patients with severe asthma: open-label extension study. Annals of medicine vol. 56,1 (2024): 2417184.
Adverse events should be reported directly to the Health Products Regulatory Authority (HPRA) on their website: www.hpra.ie.
Adverse events should also be reported to GlaxoSmithKline on 1800 244 255 or via online form https://gsk.public.reportum.com/.
© GSK group of companies or its licensor.
Trade marks are owned by or licensed to the GSK group of companies.
PM-IE-MPL-WCNT-260003 | May 2026

