

 Registrering slutförd!
Registrering slutförd! Användarkonto uppsatt – validering hanteras.
Användarkonto uppsatt – validering hanteras. Ditt användarkonto har upprättats, men vi behöver validera att du är Hälso-och sjukvårdspersonal. Vi skickar dig ett e-postmeddelande inom några dagar när validering är gjord.
Ditt användarkonto har upprättats, men vi behöver validera att du är Hälso-och sjukvårdspersonal. Vi skickar dig ett e-postmeddelande inom några dagar när validering är gjord. Under tiden kan du besöka den öppna delen av GSKs hemsida.
Under tiden kan du besöka den öppna delen av GSKs hemsida.Frequently Asked Questions
Find out answers to frequently asked questions concerning severe refractory eosinophilic asthma in adults and add-on treatment with Nucala.
About severe eosinophilic asthma
What is severe eosinophilic asthma?
Severe asthma is a heterogeneous disease comprised of different phenotypes with specific clinical and pathophysiological features. 12
Severe eosinophilic asthma is an identifiable severe asthma phenotype, characterised by eosinophilic inflammation 13
- In this condition, eosinophil levels are a useful biomarker for asthma symptoms and severity 45
- Increased numbers of blood eosinophils can be associated with severe asthma exacerbations 367
What are eosinophils?
Eosinophils are white blood cells and are activated by lymphocytes of the adaptive immune response. 7They also play a role in maintaining long-term inflammation and exacerbation risk, under the control of interleukin(IL)-5. 689
Eosinophilic airway inflammation 4

What is the role of IL-5?
IL-5 is the major cytokine responsible for the growth, differentiation, recruitment, activation and survival of eosinophils. 11
What is the difference between severe eosinophilic and severe allergic asthma?
These asthma phenotypes are distinct:
Severe eosinophilic asthma is a phenotype of severe asthma characterised by sputum and blood eosinophils, frequent exacerbations and high nitric oxide (measured using FeNO) 1-31213
Severe allergic asthma is defined as asthma with the inherited predisposition to generate immunoglobulin E (IgE) against common environmental allergens 1114
Learn more about severe eosinophilic asthma
About Nucala
What is Nucala?
Nucala is the first targeted anti-IL-5 add-on therapy for your adult patients with severe refractory eosinophilic asthma 14
How do I identify appropriate patients for Nucala?
The Nucala clinical development programme evaluated efficacy in a targeted group of patients with severe refractory eosinophilic asthma most likely to benefit from treatment using 3 criteria:
Current therapy – high-dose OCS* plus additional controller1

Exacerbation history – two or more exacerbations in the prior 12 months and/or daily OCS1

Blood eosinophil level – baseline blood eosinophils
≥150 cells/µL1**


What are the potential benefits of treatment with Nucala?
In clinical trials, Nucala added to high dose ICS and an additional maintenance treatment(s) demonstrated improvements in certain clinical endpoints vs. placebo added to high dose ICS and an additional maintenance treatment(s):
- reduced clinically significant exacerbations* by 53% reduction in exacerbation vs placebo in week 324 (0,83 vs 1,74, p<0,001) (MENSA primary endpoint, Nucala: 0.83/year, placebo: 1.74/year, p<0.001) 16
- improved quality of life (SGRQ) by 7.0 units (MENSA secondary endpoint, Nucala: -16.0 units, placebo: -9.0 units; p<0.001)† 16
- improved lung function (pre-bronchodilator FEV1) by 98mL (MENSA secondary endpoint, Nucala: 183mL, placebo: 86mL, p=0.03)† 16
- reduced daily OCS dose, while maintaining asthma control (SIRIUS primary endpoint likelihood of reduction 2.39 times greater with Nucala than with placebo, p=0.008) 17
In placebo-controlled clinical trials with Nucala (added to high dose ICS and additional maintenance treatment[s]), the rate of adverse events was similar across treatment arms, with the exception of injection site reactions (8% [21/263] for Nucala, 3% [8/257] for placebo) 7
*Clinically significant exacerbations of asthma were defined as the worsening of asthma that required use of systemic corticosteroids for at least three days or required hospitalisation and/or ED visits 17
†This secondary study endpoint is clinically meaningful, however, statistical significance cannot be inferred due to the hierarchical ‘gatekeeping’ approach used.
Learn more about the MENSA and SIRIUS study outcomes
Safety
What is the safety profile of Nucala?
A total of 915 patients with severe refractory eosinophilic asthma have received either a subcutaneous (SC) or an intravenous (IV) dose of Nucala during clinical studies of 24 to 52 weeks duration. Nucala is licensed for SC use only. 7
In placebo-controlled clinical trials with Nucala (added to high dose ICS and additional maintenance treatment[s]), the rate of adverse events was similar across treatment arms, with the exception of injection site reactions (8% [21/263] for Nucala, 3% [8/257] for placebo) 7
The most commonly reported adverse reactions during treatment were headache, injection site reactions and back pain. Systemic reactions, including hypersensitivity, were reported at an incidence comparable to that of placebo. 7
The most common symptoms associated with subcutaneous injections included: pain, erythema, swelling, itching, and burning sensation. These occurred mainly at the start of treatment and within the first 3 injections with fewer reports on subsequent injecitons. 7
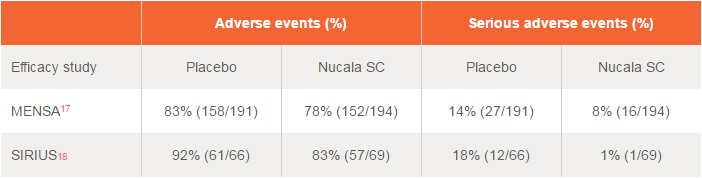
In phase III clinical trials, the incidences of adverse events (AEs) and serious adverse events (SAEs) with Nucala were found to be similar to placebo when both were added to high dose ICS and an additional maintenance treatment(s) 1617
Incidences of adverse events and serious adverse events 1617
Find out more about the Efficacy and Safety of Nucala
What were the most frequent adverse events?
In clinical studies in subjects with severe refractory eosinophilic asthma, the most commonly reported adverse reactions during treatment were headache, injection site reactions and back pain. The safety profile was similar for Nucala and placebo except for injection site reactions, which were more frequent with Nucala (8% [21/263] for Nucala, 3% [8/257] for placebo). 7
What about injection site reactions?
In clinical studies injection site reactions were more frequent in patients treated with Nucala (8% [21/263]) compared with placebo (3% [8/257]). Injection site reactions occurred mainly at the start of treatment and within the first 3 injections with fewer reports on subsequent injections. The most common symptoms associated with SC injections included: pain, erythema, swelling, itching and burning sensation. 7
Discover the potential benefits of add-on treatment with Nucala
Dosing and administration
How is Nucala administered?
Nucala is administered as a single SC injection to the upper arm, thigh or abdomen, administered once every 4 weeks. Nucala is administered with a fixed dose of 100mg(1.0mL). No weight-based adjustment is necessary. It must also be administered by a healthcare professional. 7
Find out more about how to administer Nucala
How is Nucala supplied?

How is Nucala prepared?
Nucala should be reconstituted before administration. 7
Reconstitute the contents of the vial with 1.2mL of sterile water for injection, preferably using a 2 to 3mL syringe and a 21G needle. 7
Note: the reconstituted solution must not be shaken during the procedure as this may lead to product foaming or precipitation. Reconstitution is typically complete within 5 minutes after the sterile water has been added, but it may take additional time. 7
Watch the Reconstitution Video to find out how to prepare Nucala.
For complete reconstitution and dilution instructions, visit the Dosage and Administration section of this site, or see the full Prescribing Information.
Can a patient self‐administer Nucala?
Yes, patients can self-administer Nucala. 7
How should Nucala be stored?
The shelf-life of an unopened vial of Nucala is 24 months: 7
- Store below 25°C
- Do not freeze
- Keep the vial in the outer carton in order to protect from light
References:
- Chung KF, Wenzel SE, Brozek JL et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J 2014;43(2): 343-373.
- Campo P, Rodríguez F, Sánchez-García S et al. Phenotypes and endotypes of uncontrolled severe asthma: new treatments. J Investig Allergol Clin Immunol 2013; 23(2):76-88.
- Wenzel SE. Asthma: defining of the persistent adult phenotypes. Lancet 2006; 368(9537):804-813.
- Spahn J Covar R, Stempel DA. Asthma: Addressing consistency in results from basic science, clinical trials, and observational experience. J Allergy Clin Immunol 2002; 109 (5, Supplement): S490-S502.
- Pavord I, Bafadhel M. Exhaled nitric oxide and blood eosinophilia: independent markers of preventable risk. J Allergy Clin Imunol 2013; 132(4):828–829.
- Malinovschi A, Fonseca JA, Jacinto T et al. Exhaled nitric oxide levels and blood eosinophil counts independently associate with wheeze and asthma events in National Health and Nutrition Examination Survey subjects. J Allergy Clin Immunol 2013; 132(4):821–827.
- Nucala produktresumé, fass.se
- Janeway CA Jr, et al. Immunobiology: The Immune System in Health and Disease. 5th ed. New York: Garland Science; 2001.
- Ramachandra Prahbu HD et al. JEMDS 2014; 3:5042–5047.
- Heaney LLG, Brightling CE, Menzies-Gow A et al. Refractory asthma in the UK: cross-sectional findings from a UK multicentre registry. Thorax 2010; 65(9):787-794.
- Kouro T and Takatsu K. IL-5- and eosinophil-mediated inflammation: from discovery to therapy. Int Immunol 2009; 21(12):1303-1309.
- Garcia G, Taillé C, Laveneziana P et al. Anti-interleukin-5 therapy in severe asthma. Eur Respir Rev 2013; 22(129):251-257.
- Corren J. Asthma phenotypes and endotypes: an evolving paradigm for classification. Discov Med 2013; 15(83):243–249.
- Mukherjee AB and Zhang Z. Allergic asthma: influence of genetic and environmental factors. J Biol Chem 2011; 286(38):32883-32889.
- Ortega H, Chupp G, Bardin P et al. The role of mepolizumab in atopic and nonatopic severe asthma with persistent eosinophilia. Eur Respir J 2014; 44(1):239-241.
- Ortega H, Liu MC, Pavord ID et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med 2014; 371(13):1198-1207.
- Bel EH, Wenzel SE, Thompson PJ et al. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med 2014; 371(13):1189-1197.
Nucala is a trademark of the GSK group of companies.
NUCALA (mepolizumab), 100 mg pulver till injektionsvätska, lösning, 100 mg injektionsvätska, lösning i förfylld spruta, 100 mg injektionsvätska, lösning i förfylld penna, 40 mg injektionsvätska, lösning i förfylld spruta. Medel vid obstruktiva luftvägssjukdomar, övriga systemiska medel för obstruktiva lungsjukdomar Rx (F), ATC kod: R03DX09
Terapeutiska indikationer: Nucala är indicerat som tilläggsbehandling vid svår refraktär eosinofil astma hos vuxna patienter, ungdomar och barn från 6 års ålder. Nucala är avsett som tilläggsbehandling till intranasala kortikosteroider för behandling av vuxna patienter med svår CRSwNP, som inte uppnår tillräcklig sjukdomskontroll med systemiska kortikosteroider och/eller kirurgi. Nucala är avsett som tilläggsbehandling till patienter från 6 års ålder med remitterande eller refraktär eosinofil granulomatös polyangit (EGPA). Nucala är avsett som tilläggsbehandling för vuxna patienter med otillräckligt kontrollerat hypereosinofilt syndrom (HES) utan identifierbar icke-hematologisk sekundär orsak.
Ytterligare information: I kliniska studier visades effekt hos följande subpopulation: aktuell standardbehandling som minst inkluderade högdosbehandling med inhalerade kortikosteroider (ICS) plus ytterligare en underhållsbehandling, två eller fler exacerbationer under de senaste 12 månaderna eller beroende av systemiska kortikosteroider samt blodeosinofilvärde minst 150 celler/μl vid behandlingsstart eller minst 300 celler/μl under de senaste 12 månaderna
Kontraindikationer: Överkänslighet mot den aktiva substansen eller mot något hjälpämne
Varningar och försiktighet: För att underlätta spårbarheten av biologiska läkemedel ska den administrerade produktens namn och batchnummer tydligt anges i patientjournalen. Mepolizumab ska inte användas för att behandla akuta astmaexacerbationer. Astmarelaterade biverkningar eller exacerbationer kan förekomma under behandling. Abrupt utsättning av kortikosteroider efter behandlingsstart med mepolizumab rekommenderas ej. Akuta och fördröjda systemiska reaktioner, inklusive överkänslighetsreaktioner (t.ex. anafylaxi, urtikaria, angioödem, hudutslag, bronkospasm, hypotoni), har förekommit efter administrering av mepolizumab. Patienter med befintliga maskinfektioner ska behandlas innan behandling med mepolizumab påbörjas. Om patienten blir infekterad under behandling med Nucala och inte svarar på maskmedel ska temporär utsättning av Nucala övervägas. Nucala har inte studerats hos patienter med organ- eller livshotande symtom av HES eller EGPA.
Graviditet: Som en försiktighetsåtgärd bör man undvika användningen av Nucala under graviditet. Administrering av Nucala till gravida kvinnor ska endast övervägas om den förväntade fördelen för modern är större än den eventuella risken för fostret.
Subventionsbegränsning: Subventioneras endast för patienter med svår eosinofil astma som är otillräckligt kontrollerade trots standardbehandling och antingen behandling med perorala kortikosteroider (OCS) i doser som ger ökad risk för biverkningar eller när OCS är kontraindicerat.
För fullständig förskrivningsinformation och pris, se www.fass.se.
Datum för översyn av produktresumén: 2022-10-11
GlaxoSmithKline AB, Box 516, 169 29 Solna. Tel 08-638 93 00, www.se.gsk.com.
För printmaterial lägg till nedanstående text
Om du vill rapportera en biverkning på något av våra läkemedel eller vacciner så kan du kontakta oss på följande sätt: Webformulär: se.gsk.com/biverkning. Telefon: 08-638 93 00 (be om att bli kopplad till Biverkningsenheten)
För digitalt material lägg till nedanstående text
Om du vill rapportera en biverkning på något av våra läkemedel eller vacciner så kan du kontakta oss på följande sätt: Rapportera en biverkning via webbformulär eller via telefon på 08-638 93 00 (be om att bli kopplad till Biverkningsenheten)


